⚡ Key Takeaways
- AC paracentesis instantly relieves symptoms of acutely elevated IOP
- Use a 30-gauge needle on a 1ml syringe (plunger removed)
- Bend the needle for ergonomics — bevel facing toward you creates a self-sealing incision
- The procedure is completely painless with proper topical anaesthesia
- Only a tiny amount of aqueous needs to drain — just filling the needle tip
Watch the Full Video
Why Learn This?
Patients with acutely elevated eye pressure are miserable — sweaty, restless, severe headache, nausea, vomiting. An anterior chamber paracentesis at the slit lamp can instantly relieve their symptoms. It's one of the most rewarding procedures you'll perform in clinic.
Equipment
- 30-gauge needle
- 1ml syringe
- Topical anaesthetic (tetracaine) — 2-3 drops, 5 minutes apart
- 10% betadine for disinfection
- Optional: lid speculum
Technique
Prepare the Needle
Connect the needle to the syringe, then remove the plunger. Bend the needle using its cap for better ergonomics. The direction of the bend depends on which eye you're treating.
Critical: Keep the bevel facing toward you. This creates an incision parallel to the iris that's self-sealing thanks to corneal curvature and IOP.
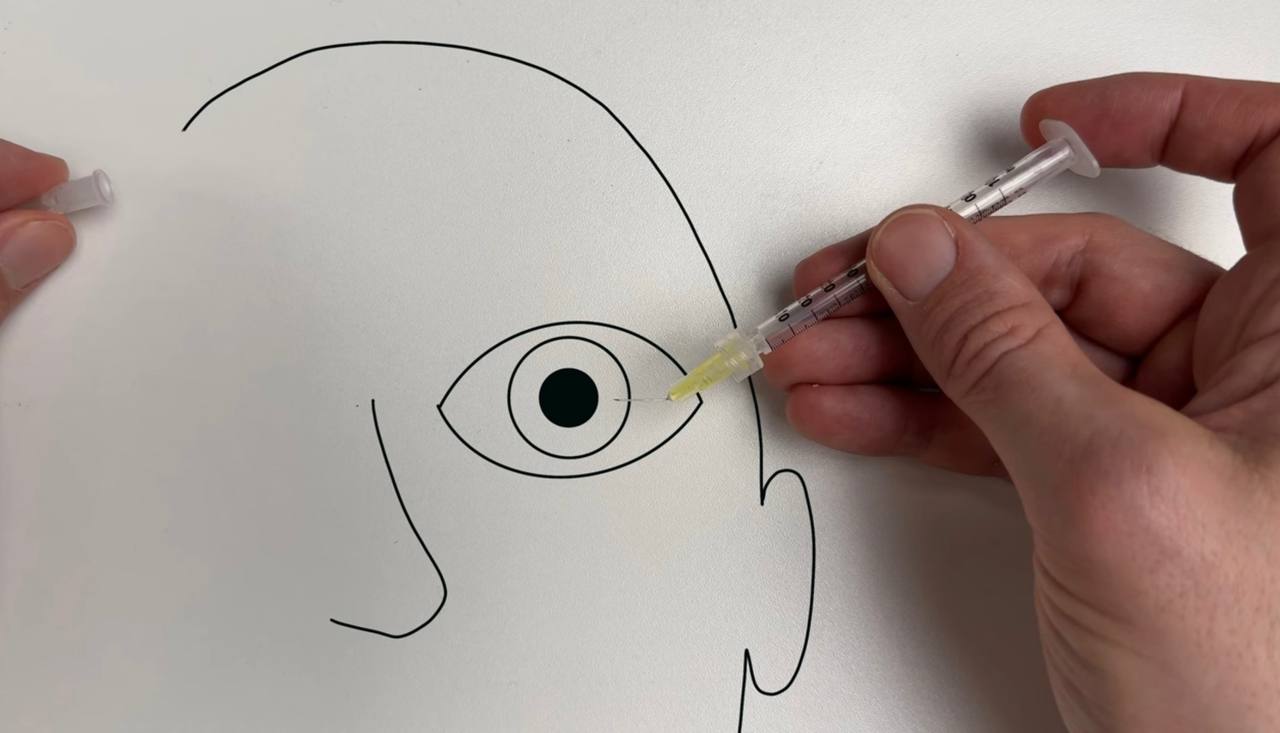
Correct needle entry technique: the bent 30-gauge needle allows for an ergonomic approach to the cornea.
Position the Patient
Ask them to look at your ear and push forward and down with their head. This stabilizes the eye. Tell them: "This is completely painless."
Perform the Paracentesis
Puncture the cornea parallel to the iris. You'll feel a little resistance, then you're through. Stay in place for a few seconds. Gently push down on the eye with the needle to estimate pressure — you'll feel it softening. Once satisfied, remove the needle.
You're not draining large volumes — usually just what fills the needle tip is enough. Check IOP afterwards. If still too high, re-enter through the same track.
Important Caveats
- Make sure the AC is deep enough — if pressure is elevated due to angle closure, the AC may be very shallow
- In a very shallow AC, you risk hitting the lens or iris — be extra careful or consider other interventions first
- The incision should be self-sealing — if it's not, you may need a bandage contact lens
Frequently Asked Questions
Is AC paracentesis safe to do at the slit lamp?
Yes. With proper anaesthesia and technique, it's a safe, quick procedure. The self-sealing incision minimizes infection risk. Use betadine disinfection beforehand.
How much fluid do you need to remove?
Very little — often just the amount that fills the needle tip (< 0.1ml). The AC volume is small, so even tiny amounts significantly reduce pressure.
Can this be done for any cause of elevated IOP?
It works best for acute angle closure, post-surgical pressure spikes, or any open-angle situation with acutely elevated IOP. Be cautious with very shallow anterior chambers or if the cause is posterior (e.g., suprachoroidal hemorrhage).
Does the pressure stay down after paracentesis?
The immediate drop is dramatic but temporary. Aqueous re-forms quickly. Use paracentesis as a bridge while definitive treatment (medication, laser PI, surgery) takes effect.
Master more clinical skills
Check out the Clinical Skills in Glaucoma course or subscribe to the YouTube channel.