⚡ Key Takeaways
- There are only two safe moments for CTR insertion: before hydrodissection (early) or after cortex removal (late)
- Early CTR requires viscodissection — not hydrodissection — to separate cortex from capsule
- Use early CTR when zonular defects are apparent at the start of surgery
- For late CTR: insert toward the zonular defect, not away from it
- Center the capsulorhexis on the lens, not the pupil, in decentered lenses
Watch the Full Video
When to Use a CTR
A capsular tension ring (CTR) stabilizes the capsular bag when zonular support is compromised. This can be due to pseudoexfoliation syndrome, trauma, or other causes of zonular weakness. The key decision is when to insert it.
Late CTR Insertion (The Classic Approach)
Most surgeons are familiar with the late approach — inserting the CTR after cortex removal. This is straightforward:
- Fill the capsular bag with cohesive viscoelastic
- Insert the CTR toward (not away from) the zonular defect — this reduces stress on the weakest area
- Use a Sinskey hook to guide the ring during insertion
- Make sure you're under the anterior capsule before releasing — otherwise the ring can spring open and stretch the rhexis
Early CTR Insertion (The Game-Changer)
Early CTR insertion is used when you can see zonular weakness from the very beginning — for example, when the lens equator is already visible before you start. In these cases, the whole lens may move during capsulorhexis.
The Key: Viscodissection
Instead of standard hydrodissection (which uses BSS), early CTR requires viscodissection. Use a cohesive viscoelastic to go under the anterior capsular edge and dissect the cortex from the capsule. The goal is to create enough space to insert the CTR without trapping cortex underneath.
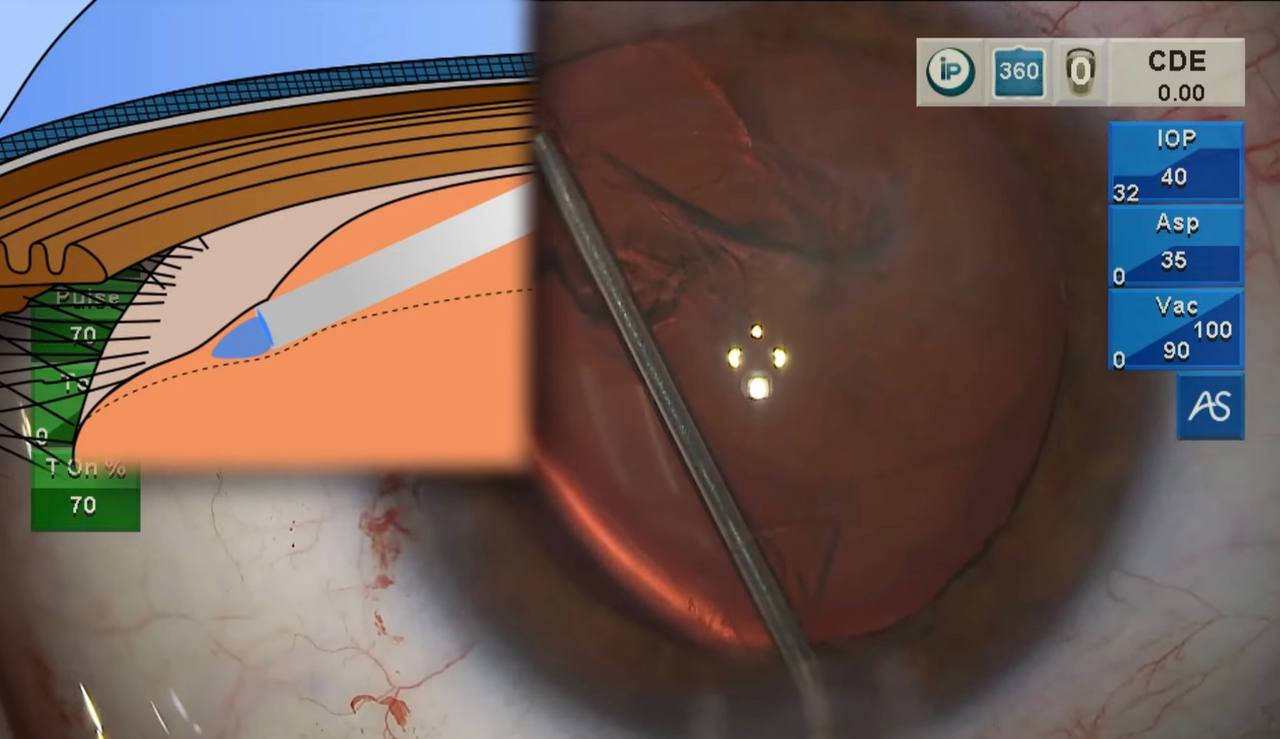
Viscodissection in action: the cannula separates cortex from capsule using cohesive viscoelastic, with an anatomical cross-section overlay.
In the beginning, you'll stir up cortex — this is normal. With practice, you'll master a clean dissection with minimal disruption. Aim for 360° dissection before inserting the ring.
Important: Center the Rhexis on the Lens
When the lens is decentered (as it often is with zonular weakness), remember to center your capsulorhexis on the lens, not the pupil. This ensures the rhexis edge provides even support around the optic after IOL implantation.
The Result
After early CTR insertion, gentle hydrodissection, phaco, and I/A, the bag is stabilized. While the bag itself may not be perfectly centered, the equator is no longer visible and the rhexis sits nicely centered on the IOL.
Frequently Asked Questions
When is early CTR preferred over late CTR?
Use early CTR when zonular weakness is obvious from the start — visible lens equator, lens movement during rhexis, or known significant pseudoexfoliation. If the weakness only becomes apparent during I/A, late CTR is your option.
What if cortex gets trapped under the CTR?
This makes I/A much more difficult. That's why thorough 360° viscodissection is critical before inserting the ring. With experience, this becomes a clean and reliable technique.
Can you use a CTR in every case of zonular weakness?
A standard CTR works for moderate zonular weakness (up to about 4-5 clock hours of defect). For more extensive weakness, consider a modified CTR with eyelet for scleral fixation (Cionni ring) or alternative fixation techniques.
Want to learn more about complex cataract surgery?
Check out the Clinical Skills in Glaucoma course or subscribe to the YouTube channel for more surgical technique videos.