⚡ Key Takeaways
- Glaucoma staging follows a 3-step process: Is it glaucoma? → What type? → What stage?
- IOP alone does not define glaucoma — progressive optic nerve damage does
- Staging is based on the visual field, not the OCT or optic nerve appearance
- The Hodapp-Parrish-Anderson (HPA) criteria use MD value and pattern of field loss
- Always correlate OCT findings with visual field defects — they should match
Watch the Full Video
A Real-World Example
Consider a patient referred with pseudoexfoliation glaucoma, IOP of 35 mmHg on four medications. The referring doctor described it as "advanced" glaucoma. But is it really? The optic nerve shows significant excavation, the OCT reveals temporal-inferior RNFL blunting — but the visual field tells a different story. There's still a lot of green and yellow. This is not advanced glaucoma.
Step 1: Is It Even Glaucoma?
High IOP alone doesn't mean glaucoma. You need evidence of optic nerve damage. The diagnostic workup includes:
- Fundoscopy — examine the optic nerve, determine cup-to-disc ratio, compare both eyes
- OCT — check RNFL thickness, GCL analysis, and minimum rim width (MRW). Do all three agree?
- Visual field — does the field defect correlate with the OCT findings?
- Progression — if available, progression data is the strongest evidence of glaucoma
Step 2: Define the Type
Once you've confirmed glaucoma, determine the type:
- Open angle vs. closed angle — gonioscopy is essential
- If closed angle: what mechanism? (pupillary block, plateau iris, etc.)
- If open angle: what subtype? (primary, pseudoexfoliation, pigmentary, etc.)
Step 3: Stage the Severity
Here's the critical point many residents get wrong: staging is based on the visual field, not the OCT. The Hodapp-Parrish-Anderson (HPA) criteria are the standard classification system.
Hodapp-Parrish-Anderson Classification
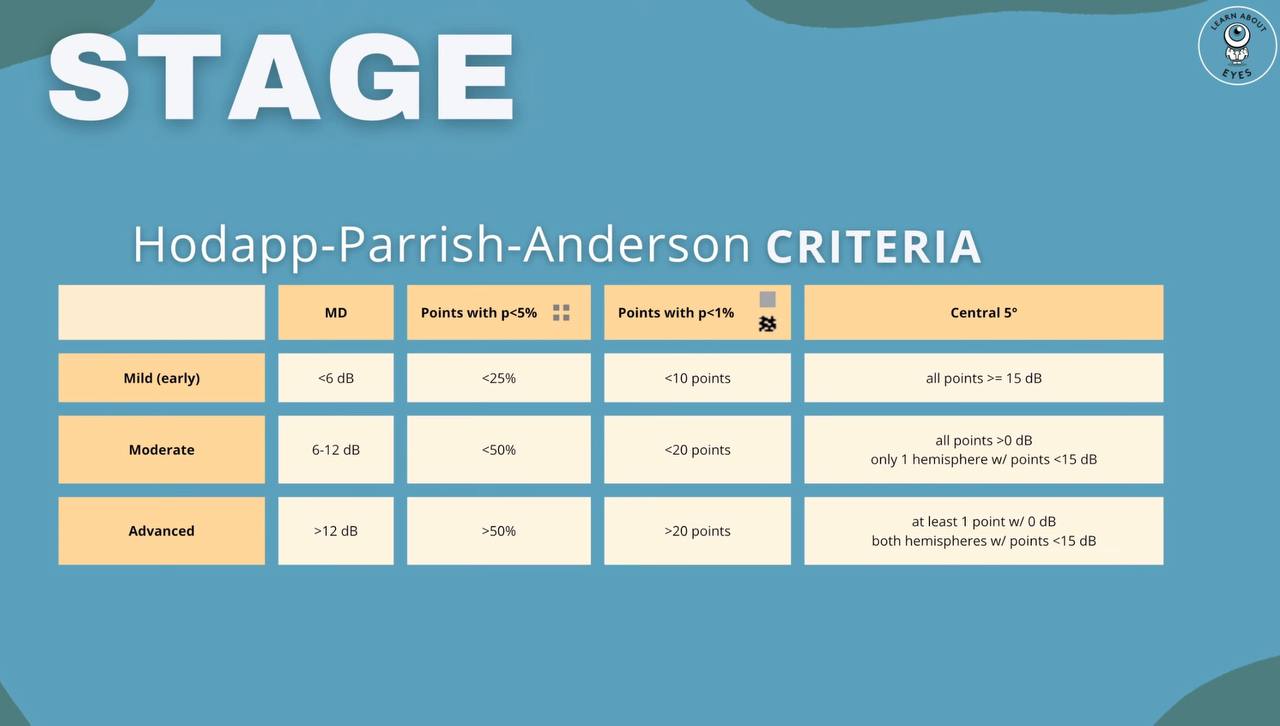
Overview of the Hodapp-Parrish-Anderson criteria for glaucoma staging.
- Mild (Early): MD better than −6 dB; fewer than 25% of points depressed below 5% level; fewer than 10 points below 1% level; no point in central 5° with sensitivity < 15 dB
- Moderate: MD between −6 and −12 dB; fewer than 50% of points depressed below 5% level; fewer than 20 points below 1% level; no point in central 5° with sensitivity of 0 dB; only one hemifield with sensitivity < 15 dB within 5° of fixation
- Severe (Advanced): MD worse than −12 dB; more than 50% of points depressed below 5% level; more than 20 points below 1% level; at least one point in central 5° with sensitivity of 0 dB; points in both hemifields with sensitivity < 15 dB within 5° of fixation
Why Staging Matters
Staging directly influences your treatment decisions. A patient with mild glaucoma and IOP of 35 has very different management than a patient with severe glaucoma and IOP of 18. The stage determines your target pressure, the aggressiveness of treatment, and how closely you follow the patient.
Frequently Asked Questions
Can OCT be used for staging instead of visual field?
No. While OCT is essential for diagnosis and monitoring, the Hodapp-Parrish-Anderson criteria are based entirely on visual field data. OCT changes often precede visual field loss, but staging relies on functional (not structural) damage.
What if the OCT and visual field don't match?
This is common in early disease (structural damage precedes functional loss) or with unreliable visual fields. Re-examine, repeat the field test, and consider other causes of field loss. In preperimetric glaucoma, the OCT is abnormal but the field is still normal.
Is the MD value alone sufficient for staging?
The MD value is a good quick screen, but the full HPA criteria also consider the pattern and location of defects, especially near fixation. A diffuse depression with MD of −8 is different from a dense arcuate scotoma with the same MD.
How often should visual fields be repeated?
In newly diagnosed glaucoma, perform 2-3 visual fields in the first year to establish a baseline and detect progression early. Stable patients can be monitored annually. Suspect progression? Repeat the field promptly.
Master glaucoma management
This topic is covered in depth in the Clinical Skills in Glaucoma online course. Subscribe to the YouTube channel for more free content.