⚡ Key Takeaways
- GAT remains the gold standard for measuring intraocular pressure (IOP)
- Master the semicircle alignment — this is where most beginners struggle
- Never push on the globe when holding lids open
- Lower magnification (6.3×) helps with the initial approach
- Always come off the cornea before adjusting the dial
Watch the Full Video
Why Learn GAT?
While there are simpler ways to measure eye pressure (like non-contact tonometry or iCare), Goldmann Applanation Tonometry remains the gold standard. Every ophthalmology resident needs to master this technique. This guide walks you through the process step by step, with tips for the most common mistakes.
Step-by-Step Guide
1. Prepare the Patient
Apply an anaesthetic eye drop combined with fluorescein dye. Some clinics have combination drops containing both agents. Warn the patient: the anaesthetic can sting briefly. Tell them the burning will go away after about 10 seconds, and give them a tissue in case the eye tears up.
2. Set Up the Measurement Tip
Take a clean measurement tip (single-use or sterilized). Slide it in so the first engraved line aligns with the white line on the measurement device. Swing the device forward on the slit lamp until it locks in place. Make sure the measurement head is straight.
3. Adjust the Slit Lamp
- Switch to cobalt blue light
- Turn brightness up to maximum
- Set the light at approximately a 45-degree angle
- Adjust until the measurement head is nicely illuminated
- Check through the eyepieces that the prism forms a straight horizontal line
4. Set Expected Pressure
On the side of the device, there's a wheel with numbers — this is where you'll read the IOP. Before measuring, set it to the pressure you expect. If you have no idea, start at around 20.
5. Approach the Cornea
Check that the eye isn't too teary (dry it off if needed). If the patient is squinting, gently hold the lids open — but never push on the globe as this falsifies your measurement.
Pull the joystick all the way back, then slowly slide the slit lamp forward while looking from the side (not through the eyepieces). Once you're close, switch to the eyepieces and use only the joystick to advance.
💡 Pro tip: If you struggle to orient yourself, lower the magnification to 6.3×. This gives you a wider field of view and greater depth of field, making the approach much less stressful. Switch back to 10× once you touch the cornea.
6. Read the Semicircles
When you touch the cornea, two fluorescent semicircles appear. What you want: two equal-sized semicircles that just touch each other on the inner edges. Do not overlap them completely.
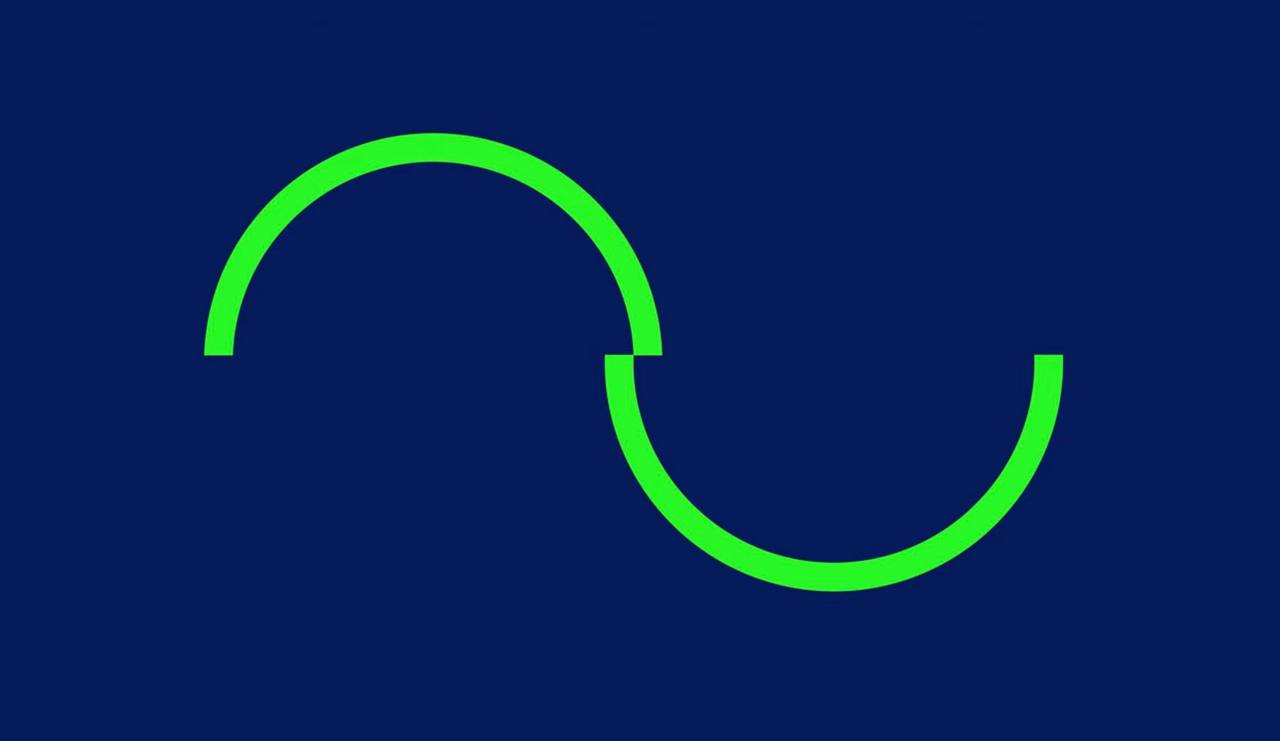
Schematic: the two fluorescent semicircles should just barely touch at their inner edges.
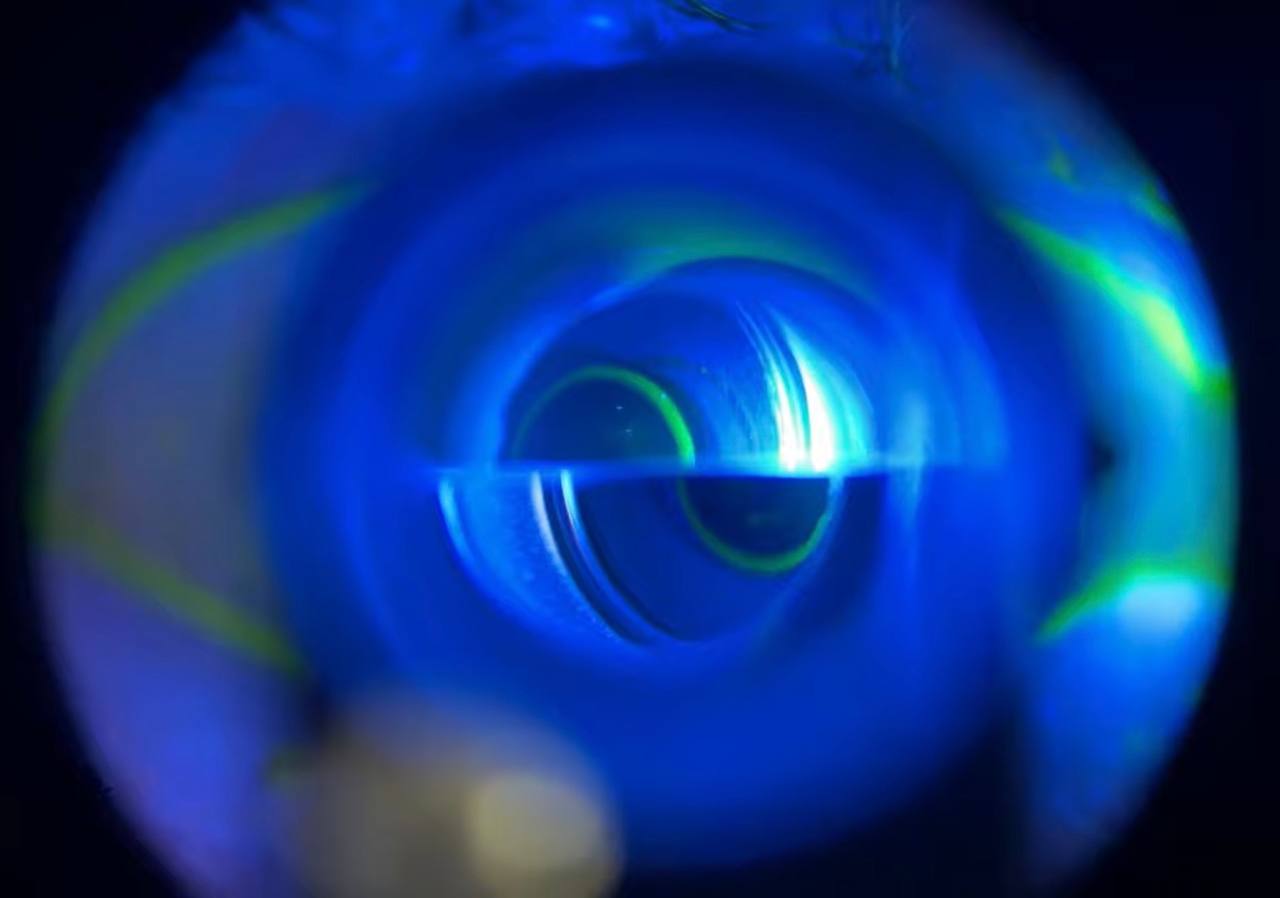
Real slit lamp view: correct alignment — the inner edges of the mires just touch, indicating accurate IOP reading.
Troubleshooting: What If It Doesn't Look Right?
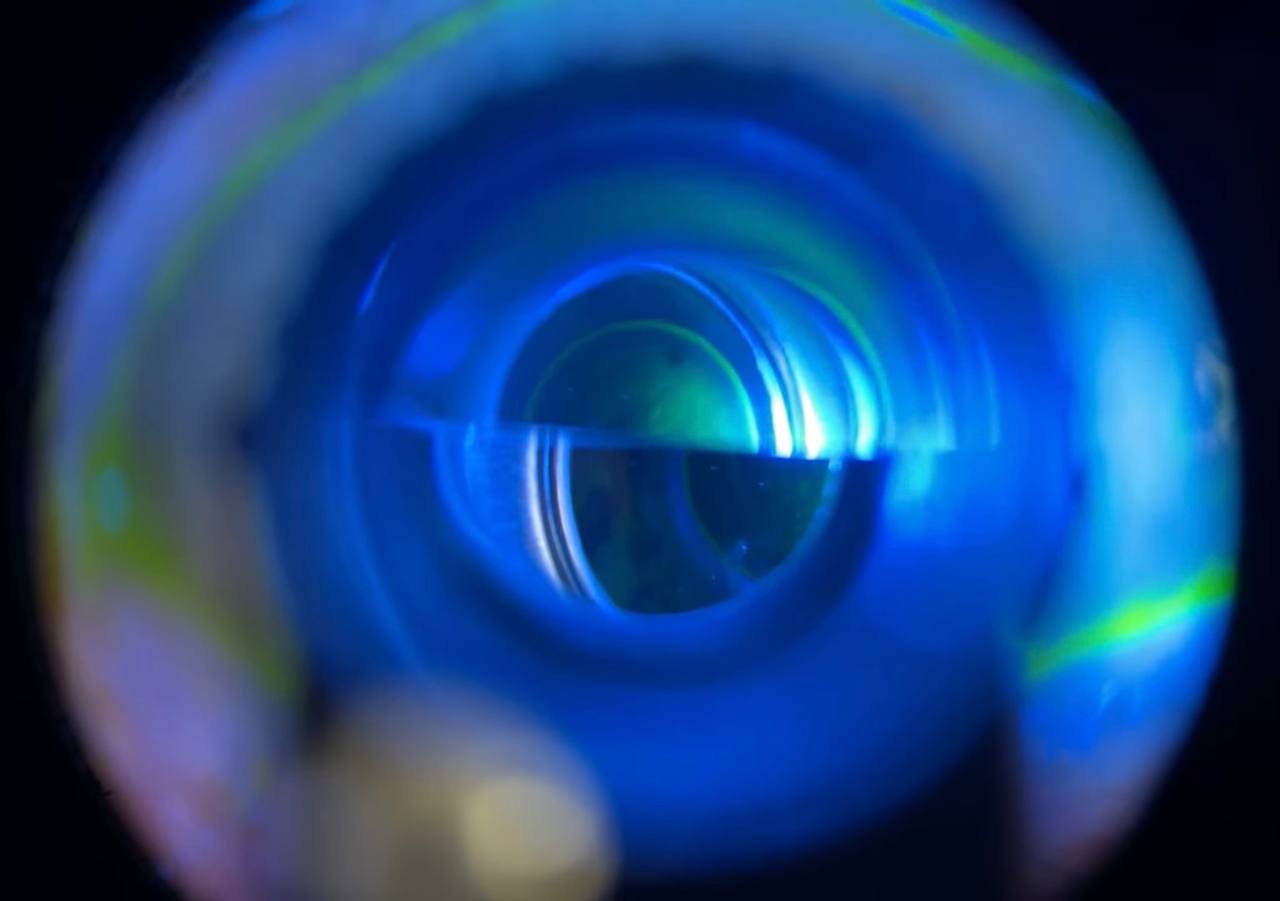
IOP lower than dial setting: the semicircles are separated and don't touch — dial down.
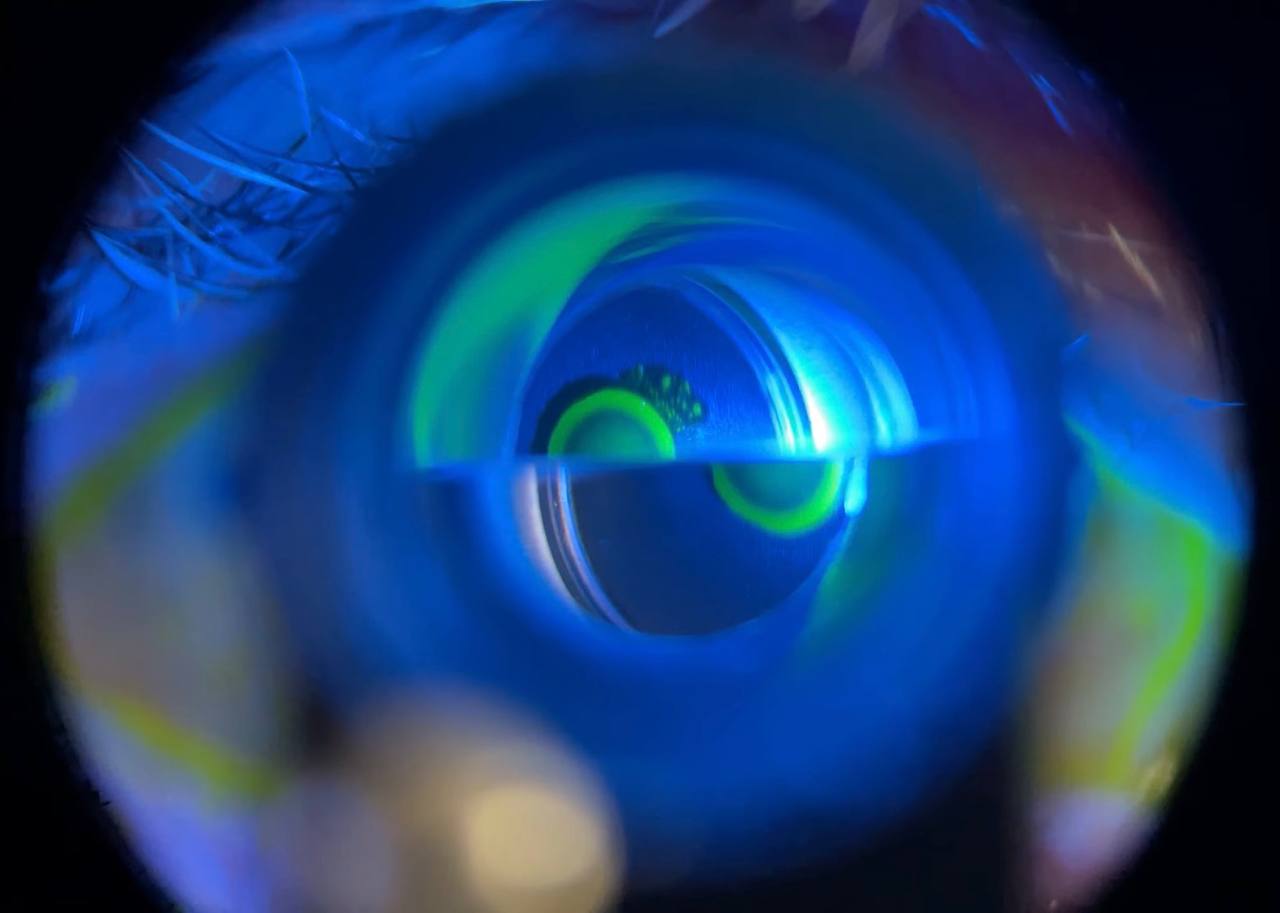
IOP higher than dial setting: the semicircles overlap excessively — dial up.
- Semicircles too small and far apart → Pressure is higher than your setting. Come off the cornea, dial up, try again.
- Semicircles too large and overlapping → Pressure is lower than your setting. Come off, dial down.
- Unequal semicircle size → You're off-center. Bigger on top? Go up. Bigger on bottom? Go down.
- One semicircle cut off to the side → Move toward the cut-off side. Come off the cornea first, reposition, re-approach.
Common Mistakes to Avoid
- Touching the cornea too lightly or too hard — find the "locked in" sweet spot
- Pressing on the globe while holding lids open
- Adjusting the dial while on the cornea — always come off first
- Too much fluorescein / tears — makes the rings too thick and unreliable
- Not warning the patient — a relaxed patient makes everything easier
Frequently Asked Questions
Is GAT painful for the patient?
No. With proper anaesthetic drops, the patient feels minimal to no discomfort. The brief contact with the cornea is painless.
How accurate is GAT compared to non-contact tonometry?
GAT is the gold standard. Non-contact (air puff) tonometry is a good screening tool but less precise, especially at higher pressures. Important clinical decisions should be based on GAT measurements.
Can I perform GAT on patients with corneal pathology?
Corneal irregularities (scarring, edema, high astigmatism) can affect accuracy. In these cases, consider alternative methods or note the limitation. This will be covered in a more detailed follow-up video.
How often should the measurement tips be replaced?
Single-use tips should be discarded after each patient. Reusable tips must be sterilized between patients to prevent cross-contamination.
Want to learn more clinical skills?
Check out the Clinical Skills in Glaucoma course or subscribe to the YouTube channel for free educational content.