⚡ Key Takeaways
- The ripcord (10-0 Nylon) is placed during surgery to stent the MicroShunt lumen and prevent early hypotony
- Removal is done at the slit lamp once the bleb has formed and IOP is stable
- Use fine forceps to grab the exposed end and pull gently in one smooth motion
- Monitor IOP closely after removal — pressure may drop significantly
- The timing of removal depends on bleb morphology and IOP trend
Watch the Full Video
What Is the Preserflo Ripcord?
The Preserflo MicroShunt is a glaucoma drainage device that diverts aqueous humor from the anterior chamber to a sub-Tenon's bleb. During implantation, a 10-0 Nylon suture can be threaded through the lumen as a "ripcord" — a stent that partially occludes flow to prevent excessive drainage and early hypotony.
When the surgeon decides the eye is ready for full flow — based on IOP trend and bleb appearance — the ripcord is removed at the slit lamp.
When to Remove
There's no fixed timeline. The decision is based on clinical judgment:
- IOP trend: Is pressure still above target despite the stent?
- Bleb appearance: Is there a healthy, diffuse bleb forming?
- Wound healing: Is the conjunctiva well-healed over the tube?
Step-by-Step Removal
- Position the patient at the slit lamp and identify the ripcord end
- Apply topical anaesthetic drops
- Using fine forceps (e.g., jeweler's forceps), grasp the exposed Nylon end
- Pull gently and steadily in the direction of the suture — one smooth motion
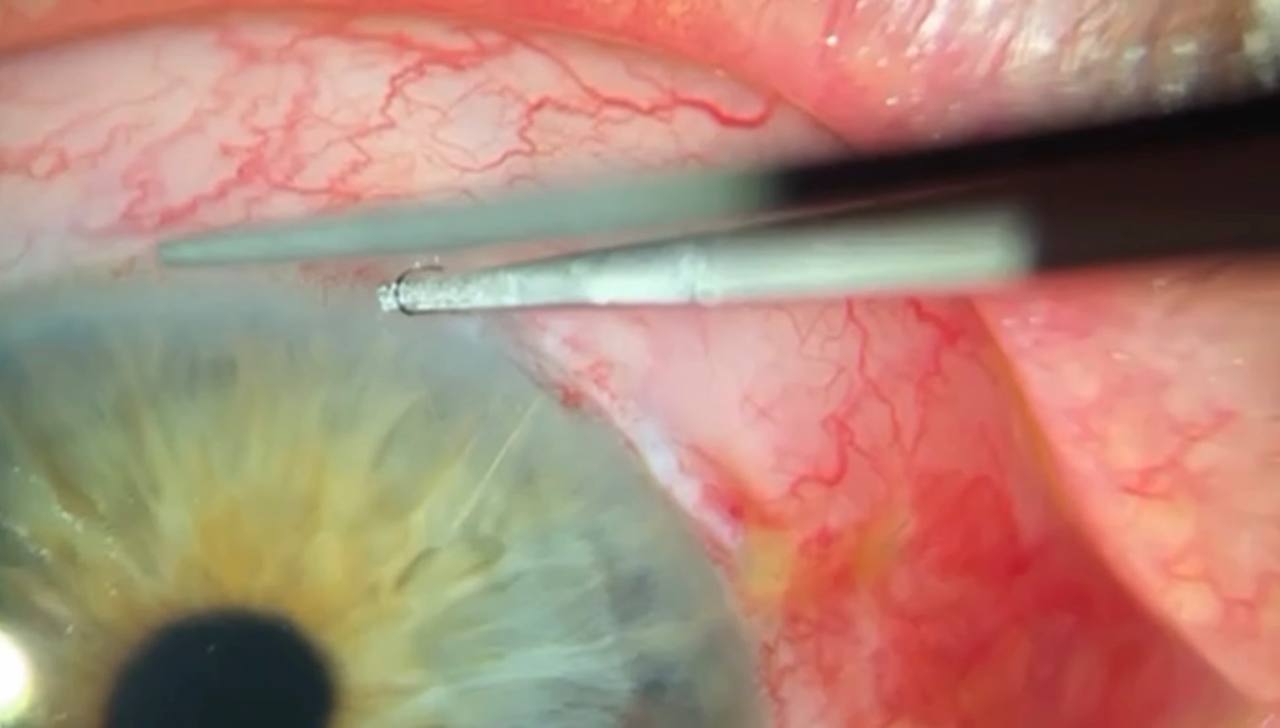
The ripcord suture being pulled from beneath the conjunctiva with fine forceps.
- Confirm the complete suture has been removed (inspect the length)
- Check IOP immediately after and at follow-up visits
Post-Removal Monitoring
After removing the ripcord, aqueous flow through the MicroShunt increases. Expect a drop in IOP. Monitor closely for hypotony (IOP < 6 mmHg) in the first days. If hypotony occurs, it usually resolves as the bleb tissue adjusts to the increased flow.
Frequently Asked Questions
Is ripcord removal painful?
No. With topical anaesthesia, patients feel minimal discomfort. The suture slides out smoothly through the MicroShunt lumen.
Can you re-stent the MicroShunt if IOP drops too low?
Once the ripcord is removed, re-stenting is not straightforward. This is why timing the removal carefully is important. Other options for managing hypotony include compression sutures or autologous blood injection.
How does this compare to laser suture lysis in trabeculectomy?
Both techniques achieve a similar goal — titrating aqueous outflow postoperatively. The ripcord technique is mechanically simpler and doesn't require a laser. The principle is the same: controlled, stepwise increase in drainage.
Learn more about glaucoma surgery
Check out the Clinical Skills in Glaucoma course or watch the Preserflo ripcord placement video.